Anorectal Malformation
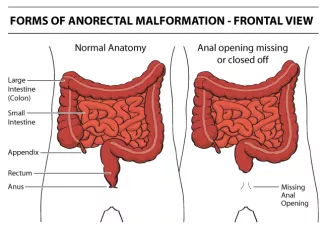
Anorectal Malformation, aka Imperforate Anus, is a spectrum of abnormalities of the rectum and anus. There are many possible abnormalities as follows:
- The absence of an anal opening.
- The anal opening in the wrong place.
- A connection, or fistula, joining the intestine and urinary system.
- A connection joining the intestine and vagina.
- In females, the intestine can join with the urinary system and vagina in a single opening, known as a cloaca.

There is no known cause for anorectal malformation and most cases are isolated and do not run in families. This birth defect occurs in one in every 5,000 live births. It is more common among Asians and is somewhat more common in boys than in girls.
What are the symptoms?
If there is a fistula (opening) to the skin, urethra or vagina, a newborn will pass meconium (a baby's first stool) and, unless a careful exam is done, the imperforate anus may not be suspected. However, if there is no anal opening and there is no fistula, the baby will not be able to pass stool after birth and this will lead to a swollen or "enlarged" abdomen and vomiting.
Since each child’s specific anatomic abnormality will vary, it is important for you to understand your child's particular anatomy.
How is the diagnosis made?
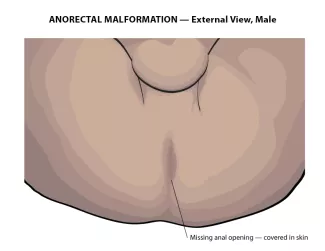
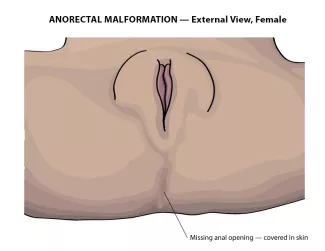
The diagnosis is made by physical examination. If the anal opening is absent or in the wrong spot, it can be seen on examination. If there is stool coming out of the urethra, or vagina, instead of the anus, it will be visible. In females with anorectal malformation, careful examination of the vestibule (area between the labia) must be made to ensure separate openings of the urethra and vagina. In the males with imperforate anus, careful examination of the perineum is necessary to identify any abnormal passage of stool.
Other associated birth defectsx
Children with anorectal malformation may also have other congenital anomalies. The following anomalies are found to occur together and are described by the acronym VACTERL association.
- Vertebral anomalies. The vertebrae are the bones of the spine and can be abnormally formed in children with imperforate anus.
- Anorectal malformation.
- Cardiac or heart defects.
- TE stands for tracheoesophageal atresia/fistula. This is an abnormality of the esophagus in which there is a blind ending or abnormal connection to the trachea (windpipe).
- Renal stands for kidney. Some children have abnormalities of the urinary system which includes kidneys, ureters, bladder and the urethra.
- Limb or abnormalities of the radial bones in the arms that lead to displaced hands.
Recommended tests
At a minimum, the following three tests are recommended.
- Cardiac echocardiogram will be needed to rule out heart anomalies.
- Renal ultrasound will be necessary to identify any urinary anomalies.
- Spine MRI will be required to rule out a tethered cord or abnormal attachment of the spine cord to the vertebrae. A untreated tethered cord may lead to bowel and bladder dysfunction.
The cardiac echo and renal ultrasound will be done at the time of the diagnosis however it is recommended to wait to perform the spine MRI until approximately 6 months of age.
What is the treatment?
In general your child will need 3 operations to correct the anorectal malformation, as determined by the anatomy: The first is to create a stoma, the second is to place the rectum through the center of the anal sphincter and the third to close the stoma. Some children will only need one operation, to place the rectum through the center of the anal sphincter. As the anatomy varies, the surgical plan will be determined after your child is carefully evaluated by the surgeon.
Skin opening in wrong location
If there is an opening for stool to drain, but it is in the wrong location, it will be placed into the correct location, within the anal sphincter. This is usually done in one operation.
No skin opening with low rectum
If there is no skin opening for stool to drain and the rectum is low and near the anal sphincter, an anal opening will be made in the correct location, within the anal sphincter. This can be done in one operation.
No skin opening with high rectum
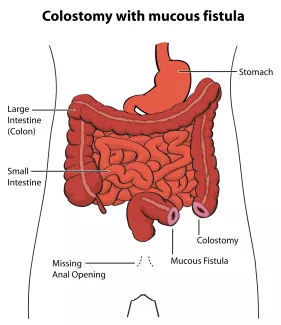
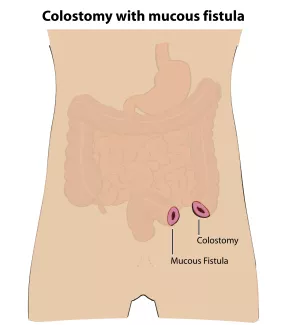
If the rectum ends high in the pelvis and is too far from the skin, surgical repair will be done in stages. First a stoma, or connection of the colon to the skin on the abdominal wall will be created.
An opening, called the colostomy, will allow stool to pass into a bag. The second opening is called the mucous fistula and allows the closed end of the rectum to drain fluid or mucous as needed. After this operation, the baby can go home to recover and grow.
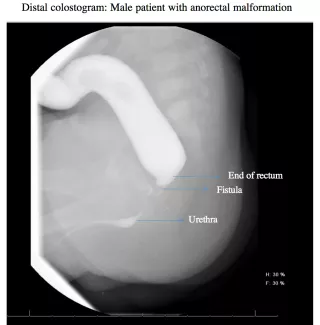
Before the second operation, where an anal opening will be made in the correct location, within the anal sphincter, your child may need to have a radiographic study called a distal colostogram to help prepare for surgery. The study helps to determine the distance from the blind end of the rectum to the skin and if there is a fistula.
If a fistula is found to the urogenital system, it will be closed at the time of the second operation. The stoma will be left intact, and not closed, to allow the new anus to heal. After this operation, the baby can go home to recover.
Two weeks after the operation to create the new anus, anal dilations will need to begin. Please refer to the section on Anal Dilations for details.
About a couple of months after the new anus is created, the stoma will be closed in a third operation. The baby will then pass stool through the new anus. It is very important to continue the anal dilations after the stoma is closed, as directed by the surgeon.
How long will my child be in the hospital after the operation?
Children can go home once they are feeding normally, having bowel movements per stoma, or anus, are comfortable on pain medication by mouth, and do not have a fever. If there is a fistula to the urinary system, a foley catheter will be placed in the bladder during the time of the operation. This allows time for the fistula closure to heal. The foley will be removed before your child goes home.
Your postoperative visit
We will make an appointment for you to bring your child to the surgeon's office for a postoperative visit two weeks after the operation. During this visit we check the stoma and/or the size of the anal opening.
When do I call the surgeon's office?
Call our office at 415-476-2538 for the following:
- Any concerns you have about your child's recovery
- A temperature of 101°F or higher
- A red incision
- Increasing pain and tenderness at the incision
- Any liquid coming out of the incision
Home Care
Babies with anorectal malformations are special babies who need special parents. They will need colon care throughout life but with personalized care, they can become very independent.
Home care immediately after surgery
Pain management
Prescription pain medication is not routinely required after hospital discharge. Most children are comfortable using acetaminophen (Tylenol®) or ibuprofen (Motrin®) at home. Follow the dosing directions on the label or use directed by your child’s doctor. If your child is still uncomfortable, call our office.
Care for incisions and dressings
Any incision on the abdominal wall may be covered with pieces of white tape called Steri-strips®. These strips fall off on their own or can be removed when they become loose. The dissolvable stitches underneath the incision may come through the incision and may be associated with a litle local redness and pus. This is normal and is best treated by gently cleansing the area with soap and water and waiting. The sutures around the stoma and the new anus will also dissolve over the next several weeks. If your child has worsening redness, swelling pain of the incision or a fever within 1–2 weeks of the operation, please call our office.
Healing Ridge
After the incisions are healed you will be able to feel a firm ridge just underneath the incision. This is called a healing ridge and it is normal to find this under an incision after an operation. The healing ridge usually lasts for several months before it softens and disappears.
Bathing Restrictions
Your child may bathe or shower between 2 and 5 days after the operation, as directed by the surgeon. Bathing may be done without restriction. The incision and the anus can be cleaned (washed and patted dry) normally. If your child has a stoma, the pouch can be removed and your child, with their stoma, can be immersed in the bath. This will not harm the stoma and is recommended. The stoma does not feel any pain and can be cleaned (washed and patted dry) and the skin around it wiped normally.
Activity Restrictions
There are no specific activity restrictions following surgery. Babies with stomas can be carried and cuddled normally.
Diaper Skin Care
Once your child starts passing stool through the new anus, very frequent bowel movements will occur and can cause severe diaper rash. Begin using a protective skin product as early as the day after surgery. A diaper rash can occur rapidly and take days or weeks to heal. Do not stop using the skin protective products until the number of bowel movements becomes less, usually after many weeks. If your child develops a rash that does not get better, please call our office. Here is a suggested routine:
- Remove all butt balm (see recipe below) cream, paste or ointment daily with mineral oil applied gently with cotton balls.
- Soak your child's bottom in a tub of warm water after applying the mineral oil.
- Clean gently with soap and water, do not scrub skin. Avoid making the skin bleed.
- At the end of the bath, pat at the skin dry.
- Apply Cavilon 3M No Sting Barrier Film by swab or spray to all affected skin in the diaper area.
- Let dry for 60 seconds
- Apply butt balm or other recommended barrier paste over the 3M product.
- After each bowel movement, clean the poop off the butt balm and do not rub the butt balm from the skin.
- Reapply more butt balm to the diaper area.
- Repeat after each bowel movement.
- Repeat mineral oil and bath routine each day.

Butt balm recipe
The recipe for butt balm is:
- four ounce tube of Desitin® ointment
- one ounce bottle of Stomahesive® powder,
- mix these two ingredients well.
These products are available in stores or online. No prescription is needed.
Colostomy care
Before your child goes home, we will teach you how to take care of your child’s new stoma and home supplies will be set up. A colostomy requires routine care to be taken when pouching (placing a bag around the stoma to collect the stool). A non-pouched colostomy requires additional instructions for management.
Anal dilation
You will receive a set of anal dilators before you leave the hospital. Bring these to your first surgical appointment. An anal incision will heal by contracting and becoming tight. If this happens, passing bowel movements will be very difficult. Stretching the anal incision gently with anal dilators is required and will begin at your child’s first postoperative visit with the surgeon. You will need to continue the dilations at home. Please follow these instructions carefully as it is essential to prevent a stricture or narrowing of the anal opening. If you are having problems with anal dilation contact the surgical nurse practitioner.
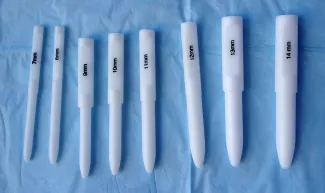
Anal dilation supplies
Dilator, K-Y lubricant, clean diaper, wipes and someone to help you, if needed.
Directions for anal dilations at home
- Position your child on his/her back, holding the feet toward the head with knees flexed.
- Lubricate the dilator and gently insert into the anus.
- Withdraw the dilator. Clean with soap and water (a very small amount of bleeding may occur, this can be normal).
- Use twice daily, for one week.
- Every week, change to a dilator that is one size larger.
- Use twice daily for one week.
- Stop increasing the size once you get to the maximum size as directed by your surgeon.
Tapering dilations
- Continue twice daily dilations for 2 weeks using dilator size as directed by surgeon.
- Decrease frequency to once daily for 2 weeks.
- Decrease to every Monday, Wednesday and Friday for 2 weeks.
- Decease to once a week for 2 weeks.
- Stop dilations.*
*Do not discard your dilators. They are to be cleaned with soap and water and saved in the event they need to be used again.
Regular follow up is recommended for bowel management of children with anorectal malformation and Hirschsprung's Disease in our LIFE clinic.
Guidelines for sizing anal dilators:
- 1-4 Months of age: 12
- 4-8 Months of age: 13
- 8-12 Months of age: 14
- 1-3 Years of age: 15
- 3-12 Years of age: 16
- > 12 years of age: 17–18
Long term care and support
Regular bowel movements, without accidents, are the goal of long term care. This can be achieved with diet modification, laxatives, and enemas.
LIFE Clinic — ARM Clinic
LIFE is an acronym for Long term Infant to adult Follow up and Evaluation Program. The LIFE Clinic provides long term care for children with birth defects including anorectal defects. Our team's expertise is based on our experience of caring for babies with imperforate anus. Your child will receive the care and attention of an experienced pediatric surgeon and nurse practitioner (NP), who have spent their careers caring for children.
To see if your child is eligible for care at the UCSF LIFE Clinic please call 415-476-2538
Parent Support Organizations
Pull-Thru Network, Inc.
http://www.pullthrunetwork.org
United Ostomy Associations of America, Inc.
http://www.ostomy.org
VACTERL Network
http://www.vacterlnetwork.org/
Infant and toddler care
Your baby's first year
Prevention of constipation is the best approach for children with anorectal malformation. Abnormal anorectal development leads to constipation and often this can be quite severe. In particular, as the baby weans from breast milk and starts taking formula and on to solids, the stools will be more bulky and bowel movements will be less frequent.
Prevention and treatment of constipation
Immediately following surgery, prevention of constipation is important for maintaining a comfortable, well adjusted and independent life. This can rarely be accomplished by diet alone. It is best achieved by softening stool with laxatives and fiber. In post-operative patients, pasty/sticky stool, very frequent or infrequent stooling, should be recognized as early signs of constipation.
Laxatives and enema therapy
In some children laxatives are not adequate to keep the child clean and enemas may be necessary, either short term or long term. Enemas are also helpful to keep the colon clean in young children with frequent stooling that leads to severe diaper rash. The timing of starting enemas is also important. Enema training may be best accepted by the child if started early in the first year of life. Enemas are often necessary for the long term colonic care for babies with imperforate anus. Sometimes, starting the enemas after one year of age can be difficult for both parent and child so an early and positive experience is helpful.
Your baby’s second year
In the second year, moderate straining is normal with bulky bowel movements. Pressing the abdomen with open palm, while the baby is straining, helps to stimulate the baby to contract the abdominal muscles reflexively to help pass a bowel movement. In time, this reflex will become a conscious effort.
Evaluation during the office visit


Abdominal Xrays are necessary to evaluate the effectiveness of the laxative or enema therapy and to identify the amount of stool in the colon. These will be done at each office visit.
Also, the surgeon or surgical nurse will determine if there is hard stool by rectal exam. If found, this can be treated by enemas or suppositories, If these fail to help the stool pass, it might be necessary to disimpact the stool in the operating room, under anesthesia.
Firm bowel movements can be painful to pass. This can lead to stool with-holding which further worsens constipation. Blood streaks lining the firm stools may mean anal fissures, which are cracks or tears near the anus caused by passing hard stools. If this is noted, increase fluid intake and call our office to schedule a clinic visit and an abdominal Xray. The dose of oral laxatives may need be increased before the clinic visit.
Adolescent and young adult care
The success of a Colonic Care Program is based on the determination and the perseverance of the young adult to be independent and responsible for his/her own well-being. The measure of success is staying clean and socially confident.
The Colonic Care Program will be tailored to the young adult's needs and consists of the following activities:
- Regularly timed voluntary bowel movement, twice a day, after breakfast and after dinner. For more read our Timed Toilet Training instructional page
- Prevention of constipation with oral laxatives.
- A daily enema program, if laxatives do not result in staying clean.
- Exercises to strengthen the abdominal muscles to maximize the Valsalva maneuver; for example, diaphragmatic breathing exercises, sit-ups, athletic sports, and calisthenics.
- Exercises to train the pelvic muscles and anal sphincters to contract. Example: pelvic squeeze and buttock squeeze.
- Relaxation techniques for pelvic muscle and anal sphincter relaxation.
- Modifying diet and eating habits, as necessary to control bowel movements.
Factors that Cause Accidental Soiling
Soiling (or accidents) may be a problem between the twice a day, timed bowel movements. There are 5 factors to consider:
- Abnormal pelvic muscles — Abnormal muscles may result from poor development, which is commonly associated with anorectal malformations. Abnormal nerves may be a result of congenital neurologic anomalies (e.g., tethered cord or spina bifida). Abnormal muscles and nerves cannot be replaced.
- Inability to sense stool — The ability to sense the presence of stool in the rectum is either present or absent and cannot be learned. If absent, conscious control of the pelvic muscles and the anal sphincters may be learned with practice.
- Chronic constipation — If your child can sense the presence of stool, problems of chronic constipation will decrease their sensation. The relief of constipation can improve this rectal sensation.
- Physical activity — Increased physical activity, particularly sports, may increase soiling. If this occurs during sports, it may be necessary to do an enema or colonic irrigation beforehand.
- The effect of certain foods — Certain foods may produce more colonic activity than others. Fried foods (burgers, French fries, chips) stimulate more activity than boiled, broiled or baked foods; sweet foods more than bland foods. Foods that are best tolerated will be learned through trial and error.
Timed Toilet Training
Timed toilet training is sitting a child on the toilet following a meal, in order to take advantage of the gastrocolic reflex, a reflex that stimulates passing a bowel movement after eating. This is started when the child is old enough to sit on the toilet, usually around age 2 to 3 years. Be patient, your child may achieve control only much later. For more read our Timed Toilet Training instructional page.
Medications
Laxatives, given by mouth, are most effective for new stool but do not soften old, dry and hard stool. Therefore they are best used to prevent constipation because soft is easier to expel than hard stool. A high dose of oral laxatives can be used to clean out a backed up colon.
The following is a summary of the types of laxatives commonly used, how they work within the intestine.
Stimulant laxatives
Stimulants work by increasing peristaltic activity (muscular contractions) of the intestinal muscles or by local irritation of the mucosal lining of the intestine. The dose we recommend will often exceed what is written on the label.
Examples are: Senna (Little Tummys, Ex-Lax, Pedia-Lax, Senokot); Bisacodyl (Dulcolax, Correctol, Bisco-Lax)
Osmotic laxatives
Osmotic laxatives retain fluid in the lumen of the colon, softening new stool.
Examples are: Polyethylene Glycol 3350 (Miralax, Glycolax); Polyethylene Glycol Electrolyte Solution (GoLYTELY; NuLYTELY).
Hyperosmotic laxatives
Hyperosmotic laxatives attract water from the bowel wall, increase intra-luminal pressure and stimulate peristalsis.
Examples are: Sorbital, Lactulose and Milk of Magnesia.
Lubricant laxatives
Lubricants coat the bowel wall and stool with a waterproof film, inhibit colonic absorption of water, and act as a lubricant to ease passage of stool.
Example: Mineral oil
Stool softeners
Softeners facilitate the mixture of fat and water to soften stool.
Example: Docusate (Colace).
Insoluble fiber (does not dissolve in water)
The unprocessed fiber found in grains, skin of fresh fruits, and vegetables. This is not absorbed and provides the bulk for producing soft stools and may be beneficial for both constipated and diarrheic stools. When processed insoluble fibers become powders and can be mixed with liquid.
Examples: Psyllium (Metamucil), Methylcellulose (Citrucel), Polycarbophil (Fibercon)
Soluble fiber (dissolves in water)
Processed fiber that is found in food such as legumes, oats, barley and fruit containing pectin (apple peel). Soluble fiber acts like osmotic laxative, absorbs water from the lumen of bowel producing soft, bulky stools.
Examples: Gaur Gum,Wheat Dextran (Benefiber ), Inulin (Fibersure) and Pectin ("Sure Jell", "Ball" or "'Certo").
Suppository
This is a medication that is inserted into the anus, in this case, to provoke a bowel movement. It can be liquid, or a solid that melts at body temperature.
Example: Glycerin (Pedialax), Bisacodyl (Ducolax).
Enemas
An enema is a treatment for constipation that involves washing out the rectum and part of the colon with water, or saline, in order to clean out stool. An enema is usually given in the anus but may also be given into a stoma. Enemas can be in low or high in volume, based on the specific recommendation for your child.
Low Volume Enemas
Low volume enemas are given using over the counter enema bottles, like the one shown in this picture. Bottles can range in size from 2 to 8 ounces. Some enema solutions contain phosphate. We recommend discarding the phosphate solution and refilling the bottle with room temperature tap water. These bottles can be cleaned and reused several times before needing to be discarded.
Sometimes the surgeon recommends adding liquid glycerin to the tap water in the low volume enema in order to make the enema more effective.
Low volume enemas are usually given as needed but in some instances are recommended to be given daily.
High Volume Enemas
Enemas are the next step when your child is unable to stay clean on laxatives and fiber alone. The successful evacuation of stool with enemas is dependent on the ability to do an effective Valsalva with relaxation of the anal sphincter in order to empty the rectum. In general, enema training should be started before the child turns 1 year old to avoid fearfulness and enema aversion.
Standard high volume enema
A standard high volume enema is given through the anus using a catheter and an enema bag. The child will be asked to hold the water or saline (as ordered by your physician) in their colon for a period of time. Detailed instructions are presented later in this section.
Retrograde enemas
Retrograde enemas are given through the anus. Antegrade continence enemas (ACE) are given through a cecostomy (stoma that connects the right colon to the skin on the abdominal wall). The cecostomy is designed to facilitate easy introduction of enema fluid (the fluid flushes the stool from the right colon and travels down into the rectum). The decision to create a cecostomy for your child depends on several factors and will require a discussion with your child’s surgeon.
Colonic irrigations
In contrast to enemas, which are given in one instillation and then evacuated, colonic irrigations consist of repeated flushing of the colon with water or saline and withdrawing the fluid (flush and withdraw) until the return flow is clear. As such, the amount needed from each day may vary. Colonic irrigations can be given retrograde or antegrade through a cecostomy. Colonic irrigations are used instead of enemas when it difficult for your child retain the enema fluid and relax the anal sphincter to empty the rectum.
Directions for administration of enemas
As you get started, it is recommended that you keep a diary of enema or irrigation details including the amount of fluid and additives, and results. This will help you track progress more effectively. It may take many weeks of practice and adjustments to get good results. The goal is for your child to be accident free (no soiling) for 24 hours, between enemas or irrigations.
Video Instructions
Gather supplies
These supplies will be ordered by the surgical nurse. Once the order is approved and filled, supplies will be sent to your home.
- Reusable enema bag (feeding bag acceptable)
- Silicone Foley Catheter — 20–24 French with 30 mL balloon for retrograde enema or 12–14 silicone Mentor catheter or extension set for MIC-KEY button or access adaptor for the Chait trapdoor cecostomy for antegrade enema
- Water soluble lubricant (for retrograde enemas only)
- 30 mL slip tip syringe (for retrograde enemas only)
- 60 mL catheter tip syringe (for retrograde only)
- Tap water or Saline as ordered by the surgical team
Getting started
- Fill enema bag with recommended volume of saline.
- For retrograde enema:
- Position your child, either bottom up or lying on the side.
- Test the balloon before using to make sure it is functional.
- Lubricate catheter and insert into anus about 4–6 inches, hold steady and inflate balloon with 10–30 mL of air to, as instructed, then pull back to secure balloon against anal opening.
- Maintain some tension on the catheter to minimize leaking.
- Attach enema bag tubing to catheter and start flow of water or saline. This should take between 5–10 minutes.
- Raising the bag will make the flow go faster, and lowering the bag will make it go slower. Proceed at a rate that is comfortable for your child.
- It is best if your child can hold the enema solution for 5–15 minutes.
- Next have your child sit on the toilet, withdraw the air from the balloon and have him or her push out the catheter (retrograde enemas only).
- For antegrade enema:
- Have your child sit on the toilet.
- Insert the catheter into the ACE stoma or attach the extension set to the MIC-KEY button or Chait tube
- Start the flow of saline
- It is recommended that your child sit on the toilet for 30–45 minutes to allow all the water/stool to be pushed out. Repeatedly doing the Valsalva maneuver will make the enema more effective.
For colonic irrigations (retrograde or antegrade):
- Insert the 20–24 french Silicone catheter into the anus or the stoma and DO NOT inflate the balloon.
- Using the catheter tip syringe, flush and withdraw the solution in 10–20 mL increments, emptying into toilet.
- Repeat until the fluid returns clear of stool.
When the enema or irrigation is completed, clean the outside of the catheter in running water and flush the inside of the catheter with the 60 mL catheter tip syringe to clear out any stool. Store for use again.
Repeat each day, at the same time.
If your child has accidents (soiling) in between each enema or irrigation, contact the surgeon or surgical nurse.
Recipe for normal saline solution
The safest normal saline solution to use is commercially prepared and purchased from a pharmacy. Saline solution can be made at home, but if mixed incorrectly using too much or too little salt, it is dangerous and can cause dehydration, seizures, lung edema or coma.
If mixing at home follow this recipe exactly:
- 1½ teaspoons table salt (never exceed this)
- 1 liter (or 1000 mL) tap water
- Stir until dissolved.
- Optional agents can be added to the saline to improve the effectiveness of the enemas. Discuss use of these additives with the surgical nurse before starting.
Colostomy Care
A colostomy requires routine care to be taken when pouching (placing a bag around the stoma to collect the stool). A non-pouched colostomy requires additional instructions for management.