Acute Liver Failure (ALF)
Acute liver failure (ALF) (also called fulminant hepatic failure) is a rare condition characterized by the abrupt onset of severe liver injury, manifest as a profound liver dysfunction as well as a confusional state called hepatic encephalopathy in individuals with no prior history of liver disease. The lack of prior liver disease is critical to the definition of ALF.
ALF vs. Acute-on-Chronic Liver Disease
Patients who suffer an acute deterioration of previously stable cirrhosis from alcohol or chronic hepatitis may have a life-threatening illness, but they do not have ALF. Unlike such patients with acute-on-chronic liver disease, patients with ALF have the potential to completely recover normal liver function, although this is far more likely with some causes of ALF than with others.
Despite its relative rarity, ALF is important because it is associated with a high mortality. However, the dismal prognosis associated with ALF appears to be improving, at least in the West. This trend likely reflects the introduction of liver transplantation as a highly effective therapy, improvement in medical intensive care, and a change in the epidemiology of ALF with a shift from causes with a relatively poor prognosis (e.g., hepatitis B) to those with a relatively good prognosis (e.g. acetaminophen overdose).
Incidence
ALF is relatively rare. The incidence of ALF is poorly defined but estimated to be approximately 2,000 cases per year in the United States, making it far less common than chronic liver disease. Approximately 6% of liver transplants in the US each year are performed on patients with ALF. There are significant geographical differences in the relative frequency of different causes of ALF across the world. In adult patients in the US, most cases of ALF are related to acetaminophen poisoning, with severe liver injury from other drugs, viral hepatitis, shock liver, and other, often undefined etiologies making up the remaining cases (see table below).
Causes
As shown in the table, a diverse array of insults can cause ALF. Liver injury from drugs and toxins is currently the most common cause of ALF in the US. Selected etiologies of ALF are discussed further below.
|
|

Acetaminophen Poisoning
Acetaminophen (one form of which is called Tylenol®) poisoning is by far the leading single cause of ALF in the US and is responsible for nearly 50% of all cases. Acetaminophen is an intrinsic, dose-dependent liver toxin, which means that if any given individual takes enough acetaminophen, they will develop severe liver injury, possible culminating in ALF (see Drug-Induced Hepatitis knol).
Of note, ALF secondary to acetaminophen poisoning may result from the intentional ingestion of a large amount of acetaminophen (as part of a suicide attempt), or from unintentional overdosing due to a so-called "therapeutic misadventure." In the latter situation, an individual taking acetaminophen for therapeutic purposes (e.g., pain or fever) unintentionally consumes excessive amounts without realizing this may cause liver damage.
Typically, patients who try to commit suicide via acetaminophen overdose and develop ALF have almost always taken greater than 10 grams (20 x 500 mg tablets) and often more than 20 grams in a single ingestion. In contrast, the unintentional overdose group usually takes smaller doses but does so several times over an entire day or over several days before presenting with ALF, so that the total dose of acetaminophen ingested is usually still quite large.
Since acetaminophen is in scores of over-the-counter cold and flu products, it is not difficult to imagine how someone with severe flu symptoms might unwittingly overdose on acetaminophen. There are also almost certainly genetic and environmental factors that affect a given person's threshold of toxicity. For example, alcohol abuse and prolonged fasting may be associated with enhanced susceptibility to acetaminophen toxicity.
Many patients with unintentional ALF also have chronic pain and take pills containing within a single tablet both acetaminophen and an opiate such as codeine. Vicodin®, a combination of hydrocodone with acetaminophen, is the most common example of this type of medication, and it is currently one of the most frequently prescribed drugs in the US.
Some patients with chronic pain who are prescribed Vicodin® and similar acetaminophen-opiate combinations, become tolerant to the opiate and need to take increasing amounts to control their pain. Addiction to these medications is also a common problem. Patients who are addicted to the opiate component, commonly crave more and more, and thereby unwittingly consume increasing amounts of acetaminophen, ultimately leading to ALF.
Although acetaminophen poisoning can cause profound liver injury, early institution of treatment with an antidote called N-acetyl cysteine (NAC) [Mucomyst®] can be life-saving. Therapy with NAC, which can be given either by mouth or by I.V. (intravenously), should be started promptly in the emergency room whenever acetaminophen overdose is suspected.
Other Medications
Scores of drugs other than acetaminophen can also produce severe liver injury (see Drug Induced hepatitis Knol). Unlike acetaminophen, however, the vast majority of these drugs produce severe liver injury very rarely and not in a dose-dependent fashion.
Mushrooms
Certain mushrooms, notably Amanita phalloides (photo), also called the "death cap", contain very potent liver toxins. Indeed, consumption of even a single mushroom may result in severe liver damage. Unfortunately, amateur mushroom pickers all too commonly mistake Amanita phalloides for an edible variety. Eating Amanita phalloides results in a classic syndrome of severe nausea, vomiting, profuse diarrhea, and crampy abdominal pain that typically begins about 8-16 hours after eating the mushrooms. Within a day or two, severe liver damage can ensue, which can be life threatening even with medical therapy. Eating wild mushrooms is thus best avoided by all but the most experienced mushroom pickers.
Viral Hepatitis
Hepatitis B
In the past, viral hepatitis B (HBV) (see Hepatitis B knol) was one of the leading causes of ALF in the US, but its incidence has been declining. It is now a rare cause of ALF in the US, accounting for about 5% of ALF cases. Hepatitis B infection may occur via sexual and parenteral transmission (e.g., from intravenous drug use).
Vertical transmission of the virus from mother to child at the time of birth may also occur; this is very common in China and other parts of Asia. Patients with vertically acquired hepatitis B may suffer reactivation of previously dormant and clinically silent hepatitis B, especially when exposed to immunosupression (for example, from chemotherapy), and a severe reactivation may culminate in an illness resembling ALF. Remember to vaccinate close contacts of HBV cases.
In such situations, treatment with nucleoside analogues (e.g., entecavir) is often tried to suppress the viral replication and reverse the ALF, but this is not always effective. Family members should be vaccinated against hepatitis B.
Hepatitis A
Compared with hepatitis B, hepatitis A causes ALF less commonly in the US. Infection with hepatitis A virus is usually transmitted by a fecal-oral route and may occur sporadically or in the setting of food or water borne outbreaks. An infamous outbreak of hepatitis A in the Pittsburgh area in 2003 resulted in more than 650 cases of hepatitis and 4 deaths from ALF. Mortality from hepatitis A increases with patient age, and that occurred in this instance. The outbreak ultimately was traced to tainted green onions used and salsa served at a local Mexican restaurant. During outbreaks of hepatitis A, it is important for close contacts of ill individuals to be treated with intravenous immunoglobulin and hepatitis A vaccine.
Other viruses, including cytomegalovirus (CMV), herpes simplex virus (HSV), and adenovirus, can rarely result in ALF, especially in immunocompromised patients such as those undergoing bone marrow transplant. Hepatitis E virus (HEV) is very rare in the US, but is a relatively common cause of ALF in certain parts of the world, including India. HEV is spread in a fashion similar to HAV. Pregnant woman infected with HEV appear to be particularly at risk for developing ALF. Hepatitis C (see HCV knol) is a very common cause of cirrhosis in the US but rarely if ever causes ALF.
Metabolic Diseases
Several metabolic diseases may affect the liver and represent rare causes of ALF. The most common metabolic disease causing ALF in adults is Wilson Disease, a rare hereditary disorder associated with abnormal accumulation of copper in the liver and other organs. Wilson disease typically effects children, adolescents, and young adults, but has been occasionally reported in older individuals as well.
Characteristically, patients with ALF from Wilson disease will present with concomitant anemia from hemolysis (red cell destruction), a brownish-green pigmented ring at the junction of the white and colored parts of the eye (the so-called Kaiser-Fleisher ring), and an unusual biochemical pattern of liver injury, which are often clues to the diagnosis. Although Wilson disease often responds to medical therapy with drugs that bind and remove copper from the body, when ALF develops the prognosis for recovery is grim, and liver transplant is usually required.
Other metabolic diseases, including alpha-1 antitrypsin deficiency and tyrosinemia, can be associated with ALF in children but are extremely rare in adults.
Other conditions
Several other conditions that affect the liver can also cause ALF.
Autoimmune Hepatitis
Autoimmune hepatitis is a relatively rare condition in which the immune system of the affected individual attacks the liver in a process that is broadly analogous to liver transplant rejection, only without the transplant. In essence, the body attacks itself.
Why this occurs is not well understood, but the condition is much more common in women than in men, similar to other autoimmune conditions like rheumatoid arthritis and lupus. Fortunately, autoimmune hepatitis usually responds to immunosuppressive therapy with steroids, but medical treatment may not be successful when the patient has advanced liver failure.
Complications of Pregnancy
ALF may rarely occur in pregnancy, usually during the last trimester and most often in patients with preeclampsia (pregnancy-associated hypertension and loss of protein in the urine). Several different forms of acute liver failure may occur in this setting. Fortunately, most patients with pregnancy-related ALF recover following expeditious delivery of the infant.
An abrupt and profound interruption of blood flow to the liver can lead to ALF, although this is rare because the liver has an unusually rich blood supply from both veins and arteries. Such so-called "shock liver" typically occurs in the setting of cardiac arrest, but can also be observed with severe heat stroke, massive tumor infiltration of the liver, or when the veins normally draining blood from the liver are blocked in a relatively rare condition called Budd Chiari Syndrome.
Indeterminate ALF
When all is said and done, after an extensive evaluation that includes blood testing, radiological studies, and often even liver biopsy, the cause of ALF in at least 15% of adult cases in the US remain enigmatic. This group, called indeterminate ALF, is probably comprised of multiple different causes, including esoteric viral infections, unrecognized toxic exposures, autoimmune and metabolic diseases.
One recent study from the Acute Liver Failure Study Group (see below) demonstrated that nearly 20% patients with indeterminate ALF had previously unrecognized acetaminophen poisoning when their blood was tested with a novel assay for acetaminophen-protein adducts present in the blood after acetaminophen overdose. This suggests that acetaminophen poisoning is an even bigger problem than previously realized.

Symptoms
Most patients who develop ALF become ill very rapidly, and the interval from onset of illness to near total liver collapse may be as short as a week or less. Often the illness will begin with nonspecific symptoms, including malaise, fatigue, nausea, and abdominal discomfort. Jaundice (yellowing of the skin) and scleral icterus (yellowing of the eyes) are often present, but may not be initially noted by patients or their families until relatively late in the course of the illness.
Encephalopathy, the cognitive dysfunction that is a sine qua non of ALF, may also initially be quite subtle. Minor changes in personality, particularly irritability, inattention, mild memory lapses, and insomnia may be the first signs. However, the severity of encephalopathy may dramatically and suddenly worsen, culminating in full-blown hepatic coma in a relatively short time.
Diagnosis
Obtaining a detailed and accurate medical history from patients with ALF can be very challenging, if not impossible, due to the presence of an altered mental status. Thus, the clinician is usually forced to rely on family and friends of the ALF patient to obtain information about recent symptoms, medication use, risk factors for viral hepatitis (e.g., intravenous drug use, recent tattoos, recent travel, exposure to other ill individuals), and any significant past medical problems.
Clues to drug-induced liver injury can sometimes be gleaned by requesting that family members or friends empty the patient's medicine cabinet into a bag and bring it to the hospital for inspection.
In addition to obtaining historical information, the medical team will perform a physical exam on the ALF patient focused primarily on determining the stage of encephalopathy, excluding stigmata of chronic liver disease, and looking for hints regarding the etiology of ALF (e.g., Kaiser-Fleisher rings in Wilson disease, as mentioned above).
Furthermore, the ALF patient will undergo extensive blood and urine testing both to grade the severity of the liver failure and to determine the etiology. Some of the testing typically performed is listed in the table below. Finally, an abdominal ultrasound is performed to assess the size, configuration, and texture of the liver, to verify that its vascular supply is intact, and to rule out masses or other problems.
_565x424.jpg)
As mentioned above, despite an extensive battery of testing, the cause of ALF in approximately 15% of adult ALF patients and almost 50% of pediatric ALF patients remains enigmatic.
Prognosis
The liver performs a myriad of vital functions including:
- processing proteins, sugars, fats, and vitamins
- removal of toxic substances (e.g., ammonia)
- production of bile acids, required for normal digestion
- synthesis of clotting factors that prevent bleeding
Thus it is not surprising that when the liver fails suddenly, the result is a devastating illness. The overall survival for ALF patients in the pre-transplant era was less than 10%. Although the survival is now much better, many patients with severe ALF still will not survive without transplant.
Thus, rapidly and accurately determining the prognosis of the ALF patient - whether his liver will spontaneously recover with medical therapy alone, or he will die without a liver transplant - is critically important. Although certain features do help determine the prognosis in ALF, such as the cause of the ALF, the severity of the hepatic encephalopathy, and certain lab tests, none is completely accurate, making the decision about whether or not to proceed with liver transplant often quite difficult.
Treatment
ALF is a medical emergency and requires prompt medical evaluation and treatment. Patients with ALF often require admission to an intensive care unit and are probably best managed in a tertiary referral center that performs liver transplantation, which can be life saving in appropriate candidates. In such centers, ALF patients benefit from care from a large and well-orchestrated team of transplant physicians and surgeons, ICU physicians and nurses, nephrologists (kidney doctors), neurologists, and possibly neurosurgeons.
The current therapy of ALF is largely supportive. The goal is to anticipate, prevent, and treat complications, and facilitate the patient's liver regeneration and repair. The most common complications, including cerebral edema, renal failure, and infection, are discussed below. Liver transplantation for ALF is also reviewed.
While as of yet there is no proven treatment for the overall ALF condition, an antidote exists for certain causes.
Common antidotes are summarized in the table below.
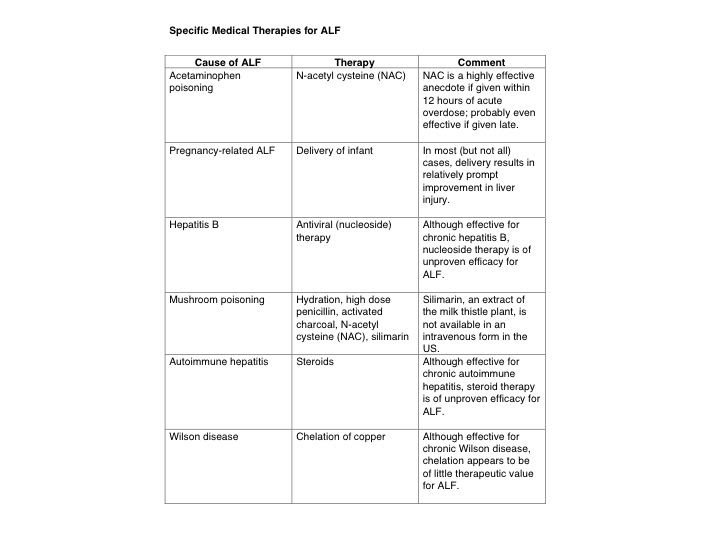
The most important antidote is N-acetylcysteine (NAC) that is used for acetaminophen poisoning. NAC is highly effective when given within 8-12 hours after acetaminophen overdose, but it loses some of its efficacy thereafter. However, it appears to be at least somewhat useful even when administered later. It may even be of some value in the treatment of non-acetaminophen ALF, although its role in this setting is still under investigation.
Cerebral Edema
Brain swelling, also called cerebral edema, is defined as a pathological increase in total brain water leading to an increase in brain volume. It is one of the most dreaded complications of ALF. Because the brain is confined to the skull, which is relatively rigid, an increase in volume rapidly translates into an increase in pressure, which in turn can cause brain damage from loss of blood flow or even life-threatening herniation, when the brain is pushed past or through a fixed structure in the skull.
The pathogenesis of cerebral edema in the setting of ALF is complex and still poorly defined, although the major brain cell type (astrocytes) and the major toxin (ammonia) involved have been identified. Patients with rapid onset ALF (for example, from acetaminophen poisoning) seem to be at particularly high risk for suffering this complication. Cerebral edema generally occurs only in ALF patients with advanced hepatic encephalopathy. In fact, most patients are in deep hepatic coma, although some display severe agitation, before this complication becomes evident.
Diagnosing cerebral edema rapidly is essential so that therapy can be started to prevent irreversible brain damage. Unfortunately, cerebral edema may be difficult to diagnose on physical exam, although some patients will develop hypertension, a slow heart rate, abnormal reflexes, and loss of the normal reaction of the pupils to light. In addition, certain findings on head CT scan, including loss of the normal junction between gray and white matter in the brain, compression of the normal fluid-filled spaces, and loss of the normal folds (sulci), are suggestive.
However, the CT scan may be normal despite high intracranial pressures, and serial CT imaging of ALF patients is not practical. Thus, many experts recommend placement of an intracranial monitor, a small device placed through the skull to measure pressure within the brain directly. This monitor, known colloquially as a "bolt", allows accurate and rapid assessment of intracranial pressure, which in turn can facilitate rapid and appropriate interventions to treat elevated pressures and prevent brain damage. However, there are significant risks associated with bolt placement, including bleeding into the brain with dire consequences. Thus, the decision to place a bolt must be individualized and rely on a carefully considered assessment of the risks and benefits for a given patient.
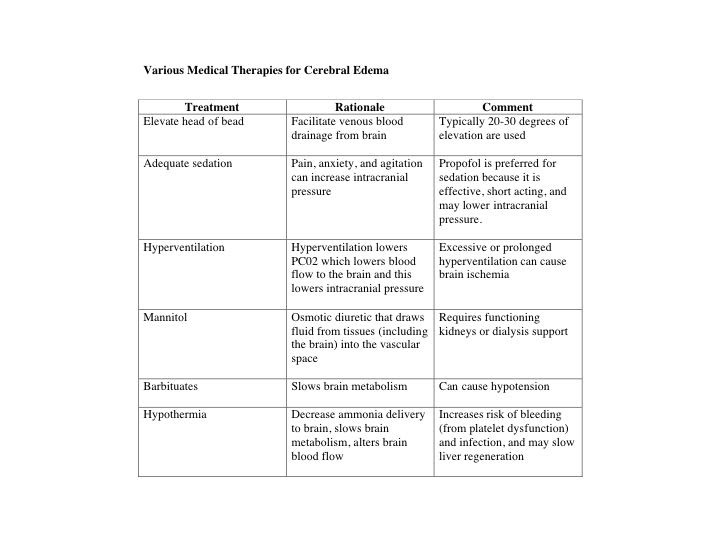
Treatments
Most of the treatments used to control cerebral edema in ALF have been borrowed from the literature on treatment of brain swelling that accompanies head trauma. Some of the treatments that are commonly used are outlined in the table below. Unfortunately, even with aggressive and appropriate therapy, cerebral edema may be unrelenting and result in profound brain injury or even brain death.
Renal failure
Renal (kidney) failure is common in patients with ALF and may be caused by a variety of factors. Studies have demonstrated that specialized, continuous forms of dialysis are superior to conventional hemodialysis in ALF patients.
Liver Transplantation
Liver transplant can be life saving for patients with severe ALF. Thus, in most cases, patients with ALF should be managed at a medical center that offers liver transplantation as a therapeutic option. If the ALF patient is not already hospitalized at a transplant program, it is important to consider early transfer to a liver transplant center, preferably one with experience managing patients with ALF. Doing so allows the patient to be evaluated by the transplant center staff to determine candidacy for liver transplant before the patient becomes too ill.
A first necessary step for liver transplant is to place the patient on the United Network for Organ Sharing (UNOS) national waiting list. In recognition of their very poor short-term prognosis, patients with ALF enjoy a special designation on the waiting list called "status 1" that equates to the highest priority for transplant possible.
As a result, patients listed for transplant with ALF essentially bypass thousands of patients with chronic liver disease who are waiting on the list, often for many months or even years. In many parts of the country, the waiting time for liver transplant for patients with status 1 listing is only 48 to 72 hours, compared with many months for those listed with chronic liver disease.
Based on current UNOS policy, the "status 1" designation requires that patients with ALF be in an intensive care unit and have either kidney or respiratory failure requiring dialysis or mechanical ventilation, respectively, or an INR > 2, a lab test measuring the clotting time that when elevated signifies severe liver failure.
Because the chances of rapidly dying with severe ALF are high, and the waiting times for transplant are unpredictable, listing appropriate patients with ALF as soon as they meet these criteria is important. Otherwise, they may develop complications that preclude liver transplantation, such as severe and untreatable cerebral edema or multi-organ failure. Obviously, patients must also meet other criteria for liver transplant candidacy (see Liver Transplant Knol).
It should be noted that, while UNOS listing is a necessary first step for liver transplant, listing is not a guarantee of liver transplant. For example, if the ALF patient develops major complications while awaiting liver transplant, such as unmanageable cerebral edema, or has contraindications to transplant (e.g., previously undiagnosed heart problems) during the pre-transplant evaluation, or spontaneously improves so that liver transplant is no longer needed, then liver transplant should not occur.
The final decision about whether to proceed with liver transplant is often made at the time a donor organ becomes available and is one of the most difficult decisions that liver transplant physicians (hepatologists) and surgeons face. Deciding to proceed with liver transplant, while potentially life saving, commits the patient not only to a major surgical procedure but also a lifetime of taking immunosuppressant and other medications. However, deciding not to proceed based on the hope that the patient's own liver will regenerate and recover, may result in a poor outcome if the patient unexpectedly takes a turn for the worse and another donor liver is not readily available.
Survival following liver transplant for ALF has historically been lower than that for chronic liver disease. However, currently one-year survivals of greater than 80% are achieved at many programs, with some larger transplant centers reporting survivals of over 90% for transplanted ALF patients.
Prevention
Since there are multiple causes of acute liver failure that all lead to essentially the same syndrome, no single measure is likely to be effective in preventing all cases. However, several measures can be envisioned that, if successfully executed, should significantly decrease the incidence of ALF in the US. For example, vaccination for hepatitis A and B has probably contributed to the declining incidence of ALF from viral hepatitis.
Public health initiatives, including guidelines regarding appropriate food handling, have likely also contributed by reducing the incidence of food-borne hepatitis A. Certainly, other areas deserve attention as well, including public education about the potential dangers of eating wild mushrooms. Finally, in the opinion of the author, legislative action directed at uncoupling acetaminophen-opiate drugs (like Vicodin®) would dramatically decrease the incidence of unintentional acetaminophen overdose (see Drug-induced Hepatitis knol), and this should therefore be a priority for the Food and Drug Administration and other regulatory agencies.
Future Developments
ALF is potentially reversible. The ALF patient's outcome depends on the balance between liver injury on the one end and liver regeneration and repair on the other. If the liver injury can be attenuated, or the liver repair and regenerative responses can be enhanced, then recovery is likely. Recent advances in molecular and cell biology have resulted in the identification of molecular targets that might soon be purposefully manipulated to tip the balance and achieve this goal.
The Acute Liver Failure Study Group consists of investigators and coordinators from 23 academic medical centers, all of which perform liver transplants, that receive support from the National Institute of Diabetes, Digestive, and Kidney Diseases to study the epidemiology, outcome and pathogenesis of ALF in the US.
Since the inception of the group in 1998, more than 1100 ALF patients have enrolled in the study, which includes a detailed clinical database as well as a serum and liver tissue bank. The group also has conducted a controlled, randomized, double blind trial of the use of an anti-oxidant, N-acetyl cysteine (NAC), for the treatment of ALF not due to acetaminophen.
Online Resources
Acute Liver Failure Study Group (ALFSG)
Drug-induced Liver Injury Network (DILIN)
Information about mushrooms and mushroom poisoning
"Mixing candy and poison" - National Public Radio/KQED - aired 10/31/05 (Halloween 2005)
"The danger of mixing candy and poison" - San Francisco Chronicle - printed 8/15/04:
* The last two links have related articles by the author arguing that acetaminophen-opiate combination drugs should be removed from the marketplace.